SURGICAL ANATOMY by JOSEPH MACLISE
COMMENTARY ON PLATES 45 & 46.
DEMONSTRATIONS OF THE ORIGIN AND PROGRESS OF FEMORAL HERNIA--
ITS DIAGNOSIS, THE TAXIS, AND THE OPERATION.
PLATE 45, Fig. 1.--The point, 3, from which an external inguinal hernia
first progresses, and the part, 5, within which the femoral hernia
begins to be formed, are very close to each other. The inguinal hernia,
3, arising above, 5, the crural arch, descends the canal, 3, 3, under
cover of the aponeurosis of the external oblique muscle, obliquely
downwards and inwards till it gains the external abdominal ring formed
in the aponeurosis, and thence descends to the scrotum. The femoral
hernia, commencing on a level with, 5, the femoral arch, descends the
femoral canal, under cover of the fascia lata, and appears on the upper
and forepart of the thigh at the saphenous opening, 6, 7, formed in the
fascia lata; and thence, instead of descending to the scrotum, like the
inguinal hernia, turns, on the contrary, up over the falciform process,
6, till its fundus rests near, 5, the very place beneath which it
originated. Such are the peculiarities in the courses of these two
hernial; and they are readily accounted for by the anatomical relations
of the parts concerned.
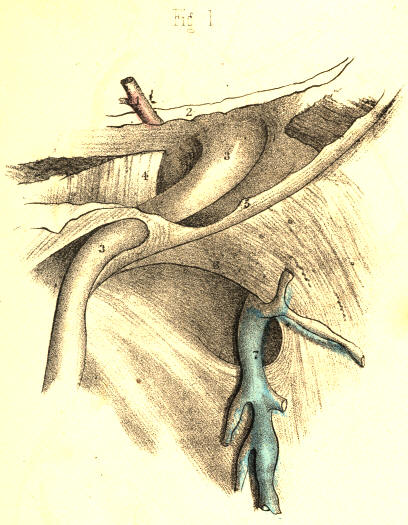
PLATE 45.--FIGURE 1
PLATE 45, Fig. 2.--There exists a very evident analogy between the
canals through which both herniae pass. The infundibuliform fascia, 3,
3, of the spermatic vessels is like the infundibuliform sheath, 9, 9, of
the femoral vessels. Both sheaths are productions of the general fibrous
membrane of the abdomen. They originate from nearly the same locality.
The ring of the femoral canal, 12, is situated immediately below, but to
the inner side of the internal inguinal ring, 3. The epigastric artery,
1, marks the width of the interval which separates the two rings.
Poupart's ligament, 5, being the line of union between the oblique
aponeurosis of the abdominal muscle and the fascia lata, merely
overarches the femoral sheath, and does not separate it absolutely from
the spermatic sheath.

PLATE 45.--FIGURE 2
PLATE 45, Fig. 3.--The peritonaeum, 2, 3, closes the femoral canal, 12,
at the femoral ring, in the same way as this membrane closes the
inguinal canal at the internal inguinal ring, 3, Fig. 2, Plate 45. The
epigastric artery always holds an intermediate position between both
rings. The spermatic vessels in the inguinal tube, 3, 3, Fig. 2, Plate
45, are represented by the round ligament in the female inguinal canal,
Fig. 3, Plate 45. When the bowel is about to protrude at either of the
rings, it first dilates the peritonaeum, which covers these openings.

PLATE 45.--FIGURE 3
PLATE 45, Fig. 4.--The place of election for the formation of any hernia
is that which is structurally the weakest. As the space which the
femoral arch spans external to the vessels is fully occupied by the
psoas and iliacus muscles, and, moreover, as the abdominal fibrous
membrane and its prolongation, the femoral sheath, closely embrace the
vessels on their outer anterior and posterior sides, whilst on their
inner side the membrane and sheath are removed at a considerable
interval from the vessels, it is through this interval (the canal) that
the hernia may more readily pass. The peritonaeum, 2, and crural septum,
13, form at this place the only barrier against the protrusion of the
bowel into the canal.

PLATE 45.--FIGURE 4
PLATE 45, Fig. 5.--The hernia cannot freely enter the compartment, 10,
occupied by the artery, neither can it enter the place 11, occupied as
it is by the vein. It cannot readily pass through the inguinal wall at a
point internal to, 9, the crural sheath, for here it is opposed by, 4,
the conjoined tendon, and by, 8, Gimbernat's ligament. Neither will the
hernia force a way at a point external to the femoral vessels in
preference to that of the crural canal, which is already prepared to
admit it. [Footnote] The bowel, therefore, enters the femoral canal, 9,
and herein it lies covered by its peritonaeal sac, derived from that
part of the membrane which once masked the crural ring. The septum
crurale itself, having been dilated before the sac, of course invests it
also. The femoral canal forms now the third covering of the bowel. If in
this stage of the hernia it should suffer constriction, Gimbernat's
ligament, 8, is the cause of it. An incipient femoral hernia of the size
of 2, 12, cannot, in the undissected state of the parts, be detected by
manual operation; for, being bound down by the dense fibrous structures
which gird the canal, it forms no apparent tumour in the groin.
[Footnote: The mode in which the femoral sheath, continued from the
abdominal membrane, becomes simply applied to the sides of the vessels,
renders it of course not impossible for a hernia to protrude into the
sheath at any point of its abdominal entrance. Mr. Stanley and M.
Cloquet have observed a femoral hernia external to the vessels.
Hesselbach has also met with this variety. A hernia of this nature has
come under my own observation. Cloquet has seen the hernia descend the
sheath once in front of the
vessels, and once behind
them. These
varieties, however, must be very rare. The external form has never been
met with by Hey, Cooper, or Scarpa; whilst no less than six instances of
it have come under the notice of Mr. Macilwain, (on Hernia, p. 293.)]

PLATE 45.--FIGURE 5
PLATE 45, Fig. 6.--The hernia, 2, 12, increasing gradually in size,
becomes tightly impacted in the crural canal, and being unable to dilate
this tube uniformly to a size corresponding with its own volume, it at
length bends towards the saphenous opening, 6, 7, this being the more
easy point of egress. Still, the neck of the sac, 2, remains constricted
at the ring, whilst the part which occupies the canal is also very much
narrowed. The fundus of the sac, 9*, 12, alone expands, as being free of
the canal; and covering this part of the hernia may be seen the fascia
propria, 9*. This fascia is a production of the inner wall of the canal;
and if we trace its sides, we shall find its lower part to be continuous
with the femoral sheath, whilst its upper part is still continuous with
the fascia transversalis. When the hernia ruptures the saphenous side of
the canal, the fascia propria is, of course, absent.

PLATE 45.--FIGURE 6
PLATE 46, Fig. 1.--The anatomical circumstances which serve for the
diagnosis of a femoral from an inguinal hernia may be best explained by
viewing in contrast the respective positions assumed by both complaints.
The direct hernia, 13, traverses the inguinal wall from behind, at a
situation corresponding with the external ring; and from this latter
point it descends the scrotum. An oblique external inguinal hernia
enters the internal ring, 3, which exists further apart from the general
median line, and, in order to gain the external ring, has to take an
oblique course from without inwards through the inguinal canal. A
femoral hernia enters the crural ring, 2, immediately below, but on the
inner side of, the internal inguinal ring, and descends the femoral
canal, 12, vertically to where it emerges through, 6, 7, the saphenous
opening. The direct inguinal hernia, 13, owing to its form and position,
can scarcely ever be mistaken for a femoral hernia. But in consequence
of the close relationship between the internal inguinal ring, 3, and the
femoral ring, 2, through which their respective herniae pass, some
difficulty in distinguishing between these complaints may occur. An
incipient femoral hernia, occupying the crural canal between the points,
2, 12, presents no apparent tumour in the undissected state of the
parts; and a bubonocele, or incipient inguinal hernia, occupying the
inguinal canal, 3, 3, where it is braced down by the external oblique
aponeurosis, will thereby be also obscured in some degree. But, in most
instances, the bubonocele distends the inguinal canal somewhat; and the
impulse which on coughing is felt at a place above the femoral arch,
will serve to indicate, by negative evidence, that it is not a femoral
hernia.

PLATE 46.--FIGURE 1
PLATE 46, Fig. 2.--When the inguinal and femoral herniae are fully
produced, they best explain their distinctive nature. The inguinal
hernia, 13, descends the scrotum, whilst the femoral hernia, 9*, turns
over the falciform process, 6, and rests upon the fascia lata and
femoral arch. Though in this position the fundus of a femoral hernia
lies in the neighbourhood of the inguinal canal, 3, yet the swelling can
scarcely be mistaken for an inguinal rupture, since, in addition to its
being superficial to the aponeurosis which covers the inguinal canal,
and also to the femoral arch, it may be withdrawn readily from this
place, and its body, 12, traced to where it sinks into the saphenous
opening, 6, 7, on the upper part of the thigh. An inguinal hernia
manifests its proper character more and more plainly as it advances from
its point of origin to its termination in the scrotum. A femoral hernia,
on the contrary, masks its proper nature, as well at its point of origin
as at its termination. But when a femoral hernia stands midway between
these two, points--viz. in the saphenous opening, 6, 7, it best exhibits
its special character; for here it exists below the femoral arch, and
considerably apart from the external abdominal ring.

PLATE 46.--FIGURE 2
PLATE 46, Fig. 3.--The neck of the sac of a femoral hernia, 2, lies
always close to, 3, the epigastric artery. When the obturator artery is
derived from the epigastric, if the former pass internal to the neck
behind, 8, Gimbernat's ligament, it can scarcely escape being wounded
when this structure is being severed by the operator's knife. If, on the
other hand, the obturator artery descend external to the neck of the
sac, the vessel will be comparatively remote from danger while the
ligament is being divided. In addition to the fact that the cause of
stricture is always on the pubic side, 8, of the neck of the sac, 12,
thereby requiring the incision to correspond with this situation only,
other circumstances, such as the constant presence of the femoral vein,
11, and the epigastric artery, 1, determine the avoidance of ever
incising the canal on its outer or upper side. And if the obturator
artery, [Footnote] by rare occurrence, happen to loop round the inner
side of the neck of the sac, supposing this to be the seat of stricture,
what amount of anatomical knowledge, at the call of the most dexterous
operator, can render the vessel safe from danger?
[Footnote: M. Velpeau (Medecine Operatoire), in reference to the
relative frequency of cases in which the obturator artery is derived
from the epigastric, remarks, "L'examen que j'ai pu en faire sur
plusieurs milliers de cadavres, ne me permet pas de dire qu'elle se
rencontre un fois sur trois, ni sur cinq, ni meme sur dix, mais bien
seulement sur quinze a vingt." Monro (Obs. on Crural Hernia) states this
condition of the obturator artery to be as 1 in 20-30. Mr. Quain
(Anatomy of the Arteries) gives, as the result of his observations, the
proportion to be as 1 in 3-1/2, and in this estimate he agrees to a
great extent with the observations of Cloquet and Hesselbach. Numerical
tables have also been drawn up to show the relative frequency in which
the obturator descends on the outer and inner borders of the crural ring
and neck of the sac. Sir A. Cooper never met with an example where the
vessel passed on the inner side of the sac, and from this alone it may
be inferred that such a position of the vessel is very rare. It is
generally admitted that the obturator artery, when derived from the
epigastric, passes down much more frequently between the iliac vein and
outer border of the ring. The researches of anatomists (Monro and
others) in reference to this point have given rise to the question,
"What determines the position of the obturator artery with respect to
the femoral ring?" It appears to me to be one of those questions which
do not admit of a precise answer by any mode of mathematical
computation; and even if it did, where then is the practical inference?]
The taxis, in a case of crural hernia, should be conducted in accordance
with anatomical principles. The fascia lata, Poupart's ligament, and the
abdominal aponeurosis, are to be relaxed by bending the thigh inwards to
the hypogastrium. By this measure, the falciform process, 6, is also
relaxed; but I doubt whether the situation occupied by Gimbernat's
ligament allows this part to be influenced by any position of the limb
or abdomen. The hernia is then to be drawn from its place above
Poupart's ligament, (if it have advanced so far,) and when brought
opposite the saphenous opening, gentle pressure made outwards, upwards,
and backwards, so as to slip it beneath the margin of the falciform
process, will best serve for its reduction. When this cannot be effected
by the taxis, and the stricture still remains, the cutting operation is
required.
The precise seat of the stricture cannot be known except during the
operation. But it is to be presumed that the sac and contained intestine
suffer constriction throughout the whole length of the canal. [Footnote]
Previously to the commencement of the operation, the urinary bladder
should be emptied; for this organ, in its distended state, rises above
the level of the pubic bone, and may thus be endangered by the incision
through the stricture--especially if Gimbernat's ligament be the
structure which causes it.
[Footnote: "The seat of the stricture is not the same in all cases,
though, in by far the greater number of instances, the constriction is
relieved by the division upwards and inwards of the falciform process of
the fascia lata, and the lunated edge of Gimbernat's ligament, where
they join with each other. In some instances, it will be the fibres of
the deep crescentic (femoral) arch; in others, again, the neck of the
sac itself, and produced by a thickening and contraction of the
subserous and peritonaeal membranes where they lie within the
circumference of the crural ring."--Morton
(Surgical Anatomy of the
Groin p. 148).]
An incision commencing a little way above Poupart's ligament, is to be
carried vertically over the hernia, parallel with, but to the inner side
of its median line. This incision divides the skin and subcutaneous
adipose membrane, which latter varies considerably in quantity in
several individuals. One or two small arteries (superficial pubic,
&c.)
may be divided, and some lymphatic bodies exposed. On cautiously turning
aside the incised adipose membrane contained between the two layers of
the superficial fascia, the fascia propria, 9, Figs. 4, 5, Plate 46, of
the hernia is exposed. This envelope, besides varying in thickness in
two or more cases, may be absent altogether. The fascia closely invests
the sac, 12; but sometimes a layer of fatty substance interposes between
the two coverings, and resembles the omentum so much, that the operator
may be led to doubt whether or not the sac has been already opened. The
fascia is to be cautiously slit open on a director; and now the sac
comes in view. The hernia having been drawn outwards, so as to separate
it from the inner wall of the crural canal, a director [Footnote] is
next to be passed along the interval thus left, the groove of the
instrument being turned to the pubic side. The position of the director
is now between the neck of the sac and the inner wall of the canal. The
extent to which the director passes up in the canal will vary according
to the suspected level of the stricture. A probe-pointed bistoury is now
to be slid along the director, and with its edge turned upwards and
inwards, according to the seat of stricture, the following mentioned
parts are to be divided--viz., the falciform process, 6; the inner wall
of the canal, which is continuous with the fascia propria, 9;
Gimbernat's ligament, 8; and the conjoined tendon, 4; where this is
inserted with the ligament into the pectineal ridge. By this mode of
incision, which seems to be all-sufficient for the liberation of the
stricture external to the neck of the sac, we avoid Poupart's ligament;
and thereby the spermatic cord, 3, and epigastric artery, 1, are not
endangered. The crural canal being thus laid open on its inner side, and
the constricting fibrous bands being severed, the sac may now be gently
manipulated, so as to restore it and its contents to the cavity of the
abdomen; but if any impediment to the reduction still remain, the cause,
in all probability, arises either from the neck of the sac having become
strongly adherent to the crural ring, or from the bowel being bound by
bands of false membrane to the sac. In either case, it will be necessary
to open the sac, and examine its contents. The neck of the sac is then
to be exposed by an incision carried through the integument across the
upper end of the first incision, and parallel with Poupart's ligament.
The neck is then to be divided on its inner side, and the exposed
intestine may now be restored to the abdomen.
[Footnote: The finger is the safest director; for at the same time that
it guides the knife it feels the stricture and protects the bowel. As
all the structures which are liable to become the seat of
stricture--viz., the falciform process, Gimbernat's ligament, and the
conjoined tendon, lie in very close apposition, a very short incision
made upwards and inwards is all that is required.]

Plate 46--Figure 3

Plate 46--Figure 4
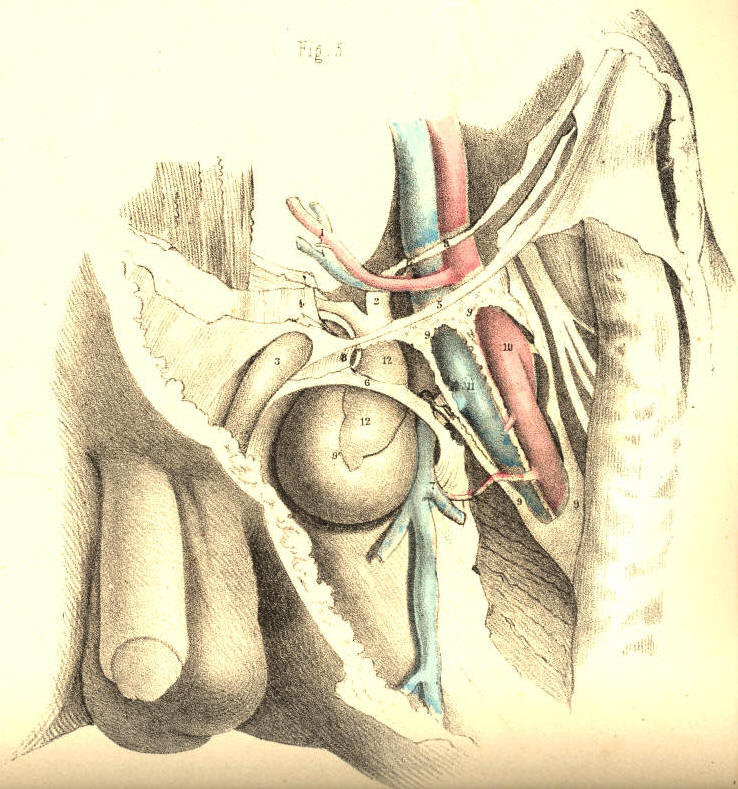
Plate 46--Figure 5
COMMENTARY ON PLATE 47